Content Warning: This essay contains statistics and stories regarding women’s sexual health. If you are wary of or upset by mentions of issues such as infertility, sexual assault, miscarriage, abortion, illness, and sex, please be aware.
Before I dig into these questions, I would like to explain why I grouped these particular topics together. I understand that some people would not have chosen to put miscarriage in the same category as abortion, and I offer sincere apologies to anyone who may be offended by that choice. I decided to put these two sensitive issues together for two primary reasons. Let me explain my thinking on this before we delve into the stats.
First of all, my decision to include miscarriage and termination in the same category is semantic. The medical language used to describe both a miscarried pregnancy and an electively terminated one is abortion. According to Dr. Karen Tang in It’s Not Hysteria, “An abortion is simply a medical term referring to the ending of a pregnancy. This includes miscarriage. When most people use the word abortion, they usually mean a situation where the pregnant person decides to end the pregnancy; that is known as elective or therapeutic abortion.” Obviously, the unintended loss of a wanted pregnancy is different than the choice to terminate an unwanted one, both in circumstance and feeling, but medically speaking, the term “abortion” applies to any end of pregnancy.
Secondly, I wanted to group these issues together because of the treatment overlap seen with miscarriages and elective abortions. With the recent fall of Roe v. Wade, medically necessary interventions are at risk in our country. In some states now, even if you lose a pregnancy that you had intended to carry to term, you may not be allowed safe access to D&C procedures or medical abortions (mifepristone or misoprostol pills) that would clear the miscarried pregnancy from the womb. In 2024, the NIH published a report called “Abortion Restrictions Threaten Miscarriage Management in the United States.” This is a telling quote from the beginning of the report:
“Restrictions on induced abortion in the US have created mounting challenges for patients requiring miscarriage care. Because miscarriage management and abortion management involve similar medications and procedures, physicians have expressed concern about oversight and sanctions for providing miscarriage support. Indeed, in states where abortion provision is criminalized, patients have experienced reduced willingness among some institutions and some clinicians to provide care, resulting in painful, traumatic, or even life- threatening experiences as people navigate miscarriages and miscarriage complications on their own.The impact of these restrictions is likely to grow over time, as the scope and quality of medical training is affected.” (NIH, 2024)
Though miscarriage and elective termination certainly have their differences, their management has many similarities. When access to these procedures is threatened, we not only prevent women the choice of ending unwanted pregnancies, we also prevent women experiencing miscarriages access to safe and expedient care.
I’ll say more on some of these things as we look at the questions, so let’s get to it.
Have you ever had a miscarriage? Yes, no, unclear

As you can see from the pie chart, most women (43) who took my survey had replied that they had never had a miscarriage. 18 women responded that they had experienced miscarriage, and 2 women replied that they were unclear. This number more or less reflects the national statistics: about 1 in 4 women experience miscarriage sometime during their life.
According to Tang, “Similar to infertility, miscarriage is extremely common. Up to 25% of recognized pregnancies end in a miscarriage. The actual rate of miscarriage is likely far higher, because many losses occur before people even know that they are pregnant. It is estimated that up to 70 percent of fertilized eggs will result in a miscarriage.” She goes on to talk about how many women are unaware that miscarriage is so common because of the perceived societal shame of losing a pregnancy. It is a heartbreaking experience, and many women may not divulge that they have lost a pregnancy with others.
I was among the majority of women on my survey who have not experienced a miscarriage. Despite not having personal experience of going through this heartbreaking loss, I have had several close friends who have experienced this, and I can attest that even as an onlooker and outside support, it is a gut-wrenching situation.
One friend of mine, who now has two beautiful children, experienced multiple pregnancy losses over a short time, several of which were traumatic and needed immediate medical intervention. During the ten years I have known her, I have watched her go through three miscarriages. She confided in me that she had had at least one prior to my friendship with her as well. Two of the three that I witnessed her experience needed quick medical care: one was an ectopic pregnancy, the other a molar pregnancy. Both these conditions can be life threatening to the mother if not addressed with expedience. All of these situations were both frightening and heartbreaking for her and her husband, and challenging for people who loved them to watch them go through.
I am grateful that my friend was able to get the life-saving care she needed, and doubly grateful that she was ultimately able to give birth to two amazing little boys. I know that each loss impacted her and her family gravely and I cannot imagine the long-term heartache, stress, and sadness that accompanies these kinds of losses. Even if a miscarriage is not traumatic, or it is the only one you ever experience, any loss of a wanted pregnancy carries with it a unique sense of grief that I can’t begin to understand. Miscarriage is a common occurrence, yes, but that does not make it an easy one for anyone who experiences it.
Have you ever terminated a pregnancy? Yes, no
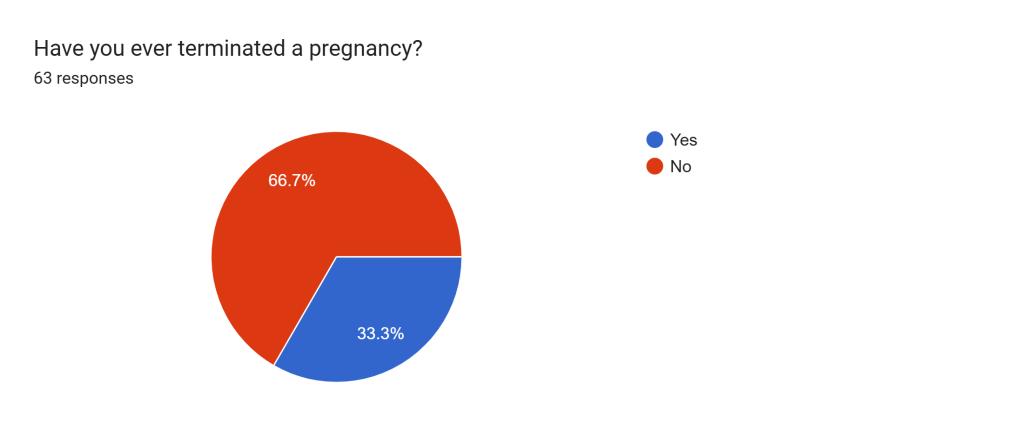
Karen Tang writes, “One in four women in the United States will have an abortion in her lifetime. Even if you aren’t personally in need of abortion care, you almost certainly know someone who has had an abortion or who will need one someday. The abortion debate ultimately has to do with people’s right to bodily autonomy and their ability to make healthcare decisions for themselves. Also, very complex medical and social factors go into the decision to end a pregnancy, and banning or criminalizing abortion can put lives at risk.” (Tang, It’s Not Hysteria)
The CDC and the Guttmacher Institute also both report that about 25% of American women under the age of 45 will receive an abortion in their lifetime. The statistics from my survey are a little over that, as you can see, with 33% of women responding that they had terminated a pregnancy (21 women total) and almost 67% saying that they had not (42 women.)
One of the books that I read that led me on this deep exploration of women’s health was called The Turnaway Study by Diana Foster Greene. It chronicles a ten-year longitudinal study on the effects of abortion access, or abortion denial, on women. She shares stories of some of the women in the study, some who received their wanted abortions, and some who did not, as well as dives into many of the pressing issues surrounding abortion, providing statistics not only from the study but also other relevant studies and reports. It is a fascinating, if sometimes heartbreaking, book and I highly recommend it. In the meantime, please check out The Turnaway Study’s website that highlights some of the key findings of Greene’s research.
One story that Greene relayed really struck me. She recalled an event that she attended with some mothers of her child’s classmates. A new mom had arrived and as one of the women was introducing her to the group, they brought her over to Greene and casually mentioned that Greene was a medical demographer, specifically studying abortion. The new mother was sort of taken aback by this and responded something to the effect of, “I just can’t imagine ever wanting to kill my baby.” Greene wrote that no one really replied and many of the mothers just got sort of quiet or awkward. A little while later, when the new mother left the function, quite a few of the women started to speak up. One mentioned that when she had been sixteen, she got pregnant, and had to get an abortion. Another brought up a story of how she had been carrying a wanted pregnancy but there were severe medical complications and so she had needed an abortion. A third then spoke up and talked about how even after her and her husband had three beautiful children, when she got pregnant with her fourth, they decided to abort because of the financial and physical strain a new baby would put on their family. And a fourth woman spoke, and a fifth, then a sixth woman. Greene was struck by how many of these women who she knew had either had abortions or been close with someone who had. The culminating thought from Greene on this story was essentially: you just don’t know how common it is, even in your own circles, because it’s not usually something women publicly share.
After reading her book and hearing this story, as well as having had a few friends who have chosen to terminate pregnancies and have confided in me about it, I was not terribly surprised to find that one third of the women who took my survey had had abortions. I do not know the circumstances of these women’s stories, and as with any of these complex and sensitive issues, I imagine the circumstances are varied. But, as Greene pointed out and the national data reflects, a lot of women have abortion stories.
Though I myself have not terminated a pregnancy, I have come a long way in how I view this issue, and I’d like to share a little bit about that journey with you. I know this is a complicated and heavy subject for a lot of people. There is a lot of grey area, and I think some people have mixed feelings or opinions about it. I want to share my personal experience on how my views on this issue have changed over the years because I hope it demonstrates that it is okay to change your mind and grow in your beliefs. I know abortion is the hot button topic so please take this caveat: what I am going to express now is purely my opinion and lived experience. Everyone is entitled to their own feelings and opinions and I recognize that this is a very personal, fraught topic for a lot of people.
As I mentioned in an earlier chapter of this essay, I was raised Catholic. For many years, I considered myself “pro-life” which at the time, for me, equated to “anti-abortion.” I still consider myself “pro-life” but have come to believe that “pro-life” and “anti-abortion” are NOT synonymous. (More on that shortly.) I remember as a teenager and even as a college student, feeling very firmly about abortion being murder, and being staunchly against it.
By the time I was in my mid-twenties, my opinion began changing. I had learned a lot more about the world and through service work, my studies, and recreational reading and learning, I began to see how complicated of an issue it truly was. For the bulk of my twenties into my early thirties I held this line: I was personally against abortion but I did not believe we lived in a world that could sustain an abortion ban and that banning or criminalizing it would cause more harm than good. I would say that if we really wanted to be a pro-life society, we need to fix the systems we live in to be able to sustain that: healthcare, education, welfare, poverty, etc. I basically identified as pro-choice because I didn’t believe we lived in a country that supported women and children enough post-pregnancy and post-birth and believed that illegalizing abortion would only make things worse.
Within the last few years, partly due to the fall of Roe v Wade, and for a cornucopia of other reasons, I have revised my stance. I am now very definitely pro-choice. Abortion is complicated and personal, and women should not have the government dictating what they can and cannot do with their bodies. I have learned a lot more about the science of conception and procreation as well and frankly, I no longer believe “life begins at conception.” I personally believe that if an embryo cannot survive outside the womb yet, it’s not a living thing. I know that this is a very contentious stance and many people would disagree. And then, some people would say it doesn’t matter, that the woman’s body and life comes first whether or not the fetus is living. To be honest, I’m not really sure how I feel about that, but I do firmly stand behind the women who choose to have an abortion for whatever reason and support their right to do so. I still think that our society needs a total overhaul, though. We are far too focused on preventing women from receiving care than creating and maintaining systems that could truly care for and support all living people.
As I said in the beginning of this little ramble, I do consider myself pro-life but for me, that does not mean I am anti-abortion. In fact, I believe that being pro-life means supporting safe abortion access. If we’re pro-life, that means caring for and protecting the women and families who are struggling and providing them with safe, accessible options. If we’re pro-life, that means we are for education reform, healthcare reform, and ending homelessness and poverty. If we’re pro-life, we are anti capital punishment in every scenario. If we’re pro-life, we are working for better solutions to combat climate change and preserve the world for the generations who will come next. If we’re pro-life, we are for much stricter gun control and we are anti-war. If we’re pro-life, we are searching for inclusive and safe solutions for the immigrant family, the trans kid, the mentally ill homeless veteran, the elderly hospice patient, the disabled mother of two, the gay couple looking to adopt, and the pregnant mother seeking an abortion. Pro-life means so much more than what people who are simply anti-abortion think it means. Let me challenge you to ask that “pro-lifer” yelling outside a Planned Parenthood about infant murder whether or not he or she believes in expanding welfare options and public education. Ask them if they believe in the death penalty. Or better yet, ask them if they own a gun.

It really grinds my gears to see these people using the term pro-life when what they truly mean is anti-abortion. There’s nothing wrong with being anti-abortion if that’s where you stand. But please, let’s just call it what it is.
Let me step down from my liberal snowflake social justice pulpit for a bit and make a few more statements about my feelings on abortion.
Two other scenarios in my life have helped me change my opinion on termination. The first, which I will get into in a little more detail in the next chapter, was when I was dating a man who was abusive. I once had a pregnancy scare while we were dating, and I remember thinking, if I’m pregnant, abortion is my only option. Though I wasn’t quite ready to get out of that relationship, I was beginning to see that things were not right. When I thought I might be pregnant with his child, it wasn’t even a question for me. I knew if that should happen, I couldn’t have the baby because that would tie me to this man for the rest of my life in some way or another, and I already knew deep down that that would be really bad. The thought came so immediately, and I think it was one of the first times I allowed myself to see some of the red flags I had been ignoring up until that point.
Recently, while reading the various books that led me to this project, I came upon some information about how women who conceive later in life are more likely to have children with chromosomal issues, like Down Syndrome. This struck a memory bubble for me. I recalled one time during early college, I was in a class and the issue of whether or not it is ethical for a woman to terminate a pregnancy if they find out their baby is going to have severe developmental delays was introduced. I remember walking away from that class incensed, thinking that I would never choose abortion just because my child was ill or had developmental disabilities. I thought it was so evil that someone would even consider abortion for that reason. Fast forward to now, 36-year-old me reading these facts with the cold terror of knowing that my husband and I, on one income and dealing with all my chronic illnesses, would likely never be able to properly care for a child with severe developmental disabilities. We may possibly strain to care for a perfectly healthy one, given our circumstances. So, if we were to conceive and then find out in the first trimester that our fetus had a severe condition that would limit not only their life but also put otherworldly, unmanageable stress on our ability to care for them and for ourselves? We would likely consider termination. I would be heartbroken, and I know we would try to figure out a way to bring the baby into our lives and care for them, but if we had no recourse to sufficiently do that, I think it is very possible that we would choose to terminate.
All this is to say that abortion is not a black and white issue. It is so very complicated on many fronts. But, it is an important medical service that we need to continue to provide in a safe and accessible way. I do not think that it is frequently a simple choice, and many people may believe it is not the right choice, but we have a responsibility to provide the opportunity for women to make that choice for themselves.
Have you ever taken Plan B or the morning after pill? Yes, no

Emergency contraception medication, often referred to colloquially as “the morning after pill” is a form of over the counter birth control, typically used after sexual intercourse has occurred. Plan B, which is the most common brand name for this medicine, consists of the hormone levonorgestrel, which is the same hormone used in many estrogen-based oral birth control medications. It works by providing a higher dose over the course of several days than typical oral contraceptives in order to interrupt any potential fertilization of eggs that could take place after unprotected sex.
According to a 2021 report by the CDC, “Among women aged 22–49 years who have ever had sexual intercourse, 24.3% have ever used emergency contraception. The percentage of women who have ever used emergency contraception increased with education level, from 12.6% among women without a high school diploma or GED to 27.9% among women with a bachelor’s degree or higher.”
My survey results reflect a slightly higher average than the national standards reported by the CDC, which may have something to do with the education levels of the women who took my survey, but it may not. 21 women responded that they had used emergency contraception; 40 women responded no they had not; and 2 women left the question blank.
I was among the 21 women who responded that they had taken Plan B. At this point in my life, I have taken this medication maybe five or six times. Typically, we think of this emergency contraception pill as something a woman takes the day after unprotected sexual intercourse because they were not careful enough at the time. This could certainly be the case, but there are many reasons that a woman may choose to take Plan B: protection could break or falter; a woman may realize that she didn’t take her oral contraceptive the day of sex or be worried that she forgot to take it or didn’t take it at the right time of day; a woman may be assaulted or raped; or a woman may just want to take it out of an abundance of caution, for any variety of reasons. Single women, partnered women, and even married women purchase emergency contraception—it is not a signal flag for a promiscuous, careless woman. It is simply a birth control measure.
The last time I personally purchased the drug was during my relationship with my husband. It was before we were married but we were already deeply committed, and possibly already living together. I had an IUD at the time but my overly cautious dearest always liked to double up on our protection during that point in our relationship. (Which is not a terrible idea, ladies. If you find a man who wants to use extra protection to ensure neither of you are at risk for situations you’re not ready for…KEEP HIM.) A moment got heated and we didn’t use our secondary form of protection as we usually did. I had had my IUD for a while and was really pretty sure we would be okay but my partner was concerned, and because good relationships are about trust and compromise, I said “okay, no problem, I will go get Plan B.” I had taken it before and hadn’t experienced any negative side effects, and it appeared to be effective as I had not yet gotten pregnant, so it wasn’t too big of a deal for me. I went to the pharmacy, purchased it, took it, and all was good in the world.

Now I would like to tell you about the first time I had to take it. Though this is a story that belongs in the following chapter, there is a piece of it that is very relevant here.
When I was a junior in college, 20 years old, I was date raped. It happened in my own apartment on our campus. My friends and I had gone out to an 18 and over night at a local dance club and met two guys from a neighboring college who ended up driving us home. They came up to our apartment for a little bit to play games. During this time, one of the men asked me to show him where the bathroom was. He lured me in with him and assaulted me. After it happened, I was sort of frozen. After they left, I ended up saying something to my roommate and she called our friend Mike, who was an RA and basically Mr. Responsible. Mike felt obliged to call Resident Services to get campus staff and the counseling center involved. At 5:30ish in the morning, after having spent about two hours in the student services office writing down what happened to me and talking to counselors in a fog, I was taken to a local hospital. Some of the resident services staff, a counselor, and my two friends went along. One of the staff members asked me if they wanted me to call anyone else to come and I requested that they call Fr. Jack, one of the Jesuit priests who worked at our campus ministry. I had recently gotten pretty close with him after attending a retreat he led only a week or so earlier.
Once at the hospital, I had a physical exam by an ER doctor and was then taken to the hospital’s rape crisis center. There, I had another physical exam, was asked a barrage of questions, surrendered my clothes for “evidence,” was swabbed all over, was photographed, and was asked by a nurse who I hope has lost her job by now, “Why didn’t you scream?”
After enduring all this with a dissociative stone-like demeanor, the nurse handed me several pills and said I had to take them. I asked her what it was and she told me—the morning after pill. At the time, I held a somewhat naive misconception about these pills and believed they were equivalent to an abortifacient. I was a practicing Catholic and at that point in my life, I was very much anti-abortion. (As you read above, my opinions on that have since changed drastically.) I told her I wouldn’t take it and she kept insisting that I had to. After a few minutes of this back and forth, I totally broke down and started to cry and loudly protest. She called the counselor to come in to talk to me. The counselor was a gentle and kind woman who said all the right things, but I had just met her a few hours previous, and at this point all the trauma of the last ten hours was catching up with me. I just wasn’t going to do another thing I didn’t want to fucking do, especially if it meant going against a religious tenet I held so firmly. How many violations of my values was I expected to permit in one day?
Right as I was reaching the peak of my emotional breakdown, the door to the exam room opened and Fr. Jack walked in. He put his arm around me, let me cry into him, and when I blubbered out that I didn’t want to take the pill and that it was the same as an abortion in my mind, he crouched down, looked me in the eyes, and told me something I will never forget.
He told me I was wrong. He gently explained to me the science of the pill and of conception and told me that there hadn’t been enough time yet for any life to exist inside of me or for fertilization to take place, but that because of the risk, I would be smart to take the pill. He told me that what had happened to me was “not of God” and that God wouldn’t want me to carry the sin of the man who had hurt me. He encouraged me to take the morning after pill. In fact, he more or less told me that I had to take it. But unlike the crisis center nurse, he corrected my misgivings, explained away my worries, comforted me, prayed with me, and held me while I took the medicine.
Yes, kids, you heard it right—a Catholic priest insisted I take the morning after pill. Thank God for the Jesuits, seriously.
This interaction had a giant impact on me for many reasons. It certainly helped change the way I perceived emergency contraception. And boy did it make me appreciate the Jesuits even more.

The last thing I would like to say about Plan B is this: I have come to see it as what it is, simply a format of birth control. Is it more responsible to cover your ass ahead of time? Sure. Does that always work or always happen in the heat of the moment? No. So thank God there’s a solution for those situations.
I will say, though I haven’t purchased it in maybe six or seven years so this may have changed, the way it is sold is preposterous. In my experience, it is available at any CVS or Walgreens or other commercial pharmacy but is typically behind the front desk, like cigarettes and lottery tickets. Not at the pharmacy or in the feminine care or sexual health aisles where you can find pregnancy tests, condoms, and lubricant, among other things, but behind the front desk with the usually male, often non-fluent English speaking, non-pharmacist cashier. The first couple times I went to purchase it, I felt ashamed and the brusque non-medically trained cashiers did nothing to make me feel any better. Why it is not available in the aisle or even at the pharmacy counter is beyond me. It’s a safe assumption that some women who come in to purchase this may be feeling awkward or nervous and having to go up to the front and ask a dude to get it for you in front of the whole line behind you can really add to any embarrassment or confusion a woman may already be feeling about buying it. If I can grab a paternity test, magnums, a raunchy magazine, a case of beer, and a box of heavy flow tampons and head discretely to self checkout, I should be able to do the same with Plan B pills. It’s not like it’s addictive or something someone would want to sell on the black market—it’s legitimately just estrogen pills. I think we can make the purchasing of this a little easier, less potentially embarrassing, and more accessible for women who choose to use it.
Have you used any form of birth control during your life? Yes, no

As you can tell from this pie chart, a sweeping number of women who took my survey have used some type of birth control during their lives. 60 women said yes, and 3 women said no. Let’s look at the next question, delving into the different types of contraceptive methods women may choose to use, before we get into some more information on birth control in general.
If so, what forms? Select all that apply. Condoms or diaphragms, birth control pill, IUD, implants or patches, surgical sterilization of self or partner, other

I provided six options on the survey that women could select. The options were: condoms or diaphragms; birth control pill; IUD; implants or patches; surgical sterilization of self or partner; and other. 51 women answered they had used condoms or diaphragms; 48 women answered they had used the birth control pill; 14 women answered that they had used surgical sterilization of self or partner; 11 women answered they had used IUDs; 8 women answered they had used other forms of birth control; and 7 women answered they had used implants or patches.
Compared to CDC data gathered between 2022 and 2023, my survey results are strikingly over the average. As you can see from the CDC graph below, 54.3% of females between the ages of 15-44 were found to use some form of contraception, and a whopping 45.8% were found not to be using any form of contraception.
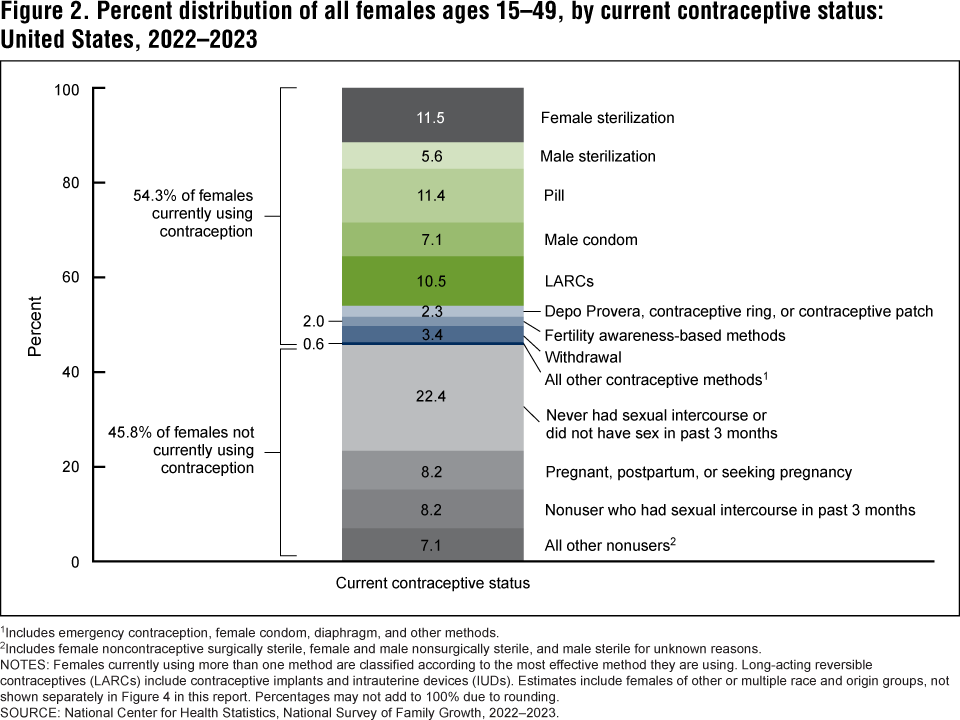
I was surprised to see that female sterilization is the highest preferred method on this graph, but that may have something to do with the age of the women who responded. In other data I found from this same CDC report, female sterilization is most popular with women ages 40-49, whereas the pill, and long-acting reversible contraception methods such as IUDs, patches, and implants were most popular with women ages 20-29 and 30-39.
It did not surprise me to find that on my survey, the two most popularly used birth control options were condoms/diaphragms and the birth control pill. Both of these options are widely available and relatively safe. Obviously, if you are attempting to protect yourself or your partner from any unknown factors including sexually transmitted infections, condoms or diaphragms are the way to go. The birth control pill, though popular, is probably the riskiest form of medicinal birth control simply because its mechanism makes the opportunity for user error so easy. For anyone who has not been on a regular oral contraceptive, let me sum up. You have to take these tiny estrogen or progesterone pills every day, at the same time, like clockwork. Should you miss a dose or largely skew the time that you take your daily dose, you’re advised to “double up” on protection. Seems easy, no problem, but let me tell you: it’s not always that easy. Plus, many estrogen birth control pills cause an array of side effects. Some women do better on progesterone only pills, which can also work, but they have the same scheduling caveats as their more typical estrogen-heavy cousins.
Long-acting reversible contraceptive medications and devices include IUDs (intrauterine device) which can be hormonal or non-hormonal (usually copper); implants; hormone injections; contraceptive rings; and patches. These methods have the benefit of being 92% to 99% effective as well as something you can forget about for a while once you have it. The downside of these methods is that some require minor medical procedures (IUD insertion or implant insertion) or repeated visits to a doctor’s office to receive injections. For some women, these long-acting methods are very useful, and if your goal is preventing pregnancy, they are extremely effective.
Like most of the women on my survey, I have used multiple forms of birth control throughout my life including the pill (both the estrogen and progesterone only varieties), an IUD, condoms, and “other.” When I said this to my husband recently, his response was “What other? The pullout method?” I cackled hysterically because he knows me so well. There are probably a variety of “other” methods I did not list but yes, indeed, that is what I meant when I selected “other.” Not a great idea by any means ladies, but I know I am not the only one out there who put “other” and was thinking of this. Hey, shit happens. We all get it. In all seriousness though, there are way safer, more surefire ways to prevent pregnancy, and if that is your goal, you should definitely find a more consistent solution.
Though I am currently on a progesterone only pill, I take this medication less for actual contraceptive reasons, but as part of managing my endometriosis. (I will be getting more into that in the last chapter.) For me, the best form of birth control was the IUD. It was painful as hell to get it inserted and to have it removed, but in between it worked incredibly effectively. I liked that I didn’t have to think about it or worry if I took my medicine at the right time every day. I ended up having it taken out before it expired because I had a fluke situation where it dislodged and was stuck in the wall of my uterus (super painful) and though that could happen to anyone, I do not believe that is a frequent occurrence. Different things work for everyone though, and the important thing is you find a method that works for you.
The last thing I’ll say about birth control: don’t ever let a man push you into any kind of method you are uncomfortable with. If you are opposed, for any reason, to going on hormonal birth control but your boyfriend is really eager to not wear a condom anymore, get a new boyfriend. Seriously. Or you can explore some other contraceptive methods out there, too. But the thing is, if a man truly loves you and wants to be with you, even if wearing a prophylactic “doesn’t feel as good,” he will wear a damn condom if you don’t want to get on a medication you are nervous about. No good partner will force you to do something you don’t want to do even if it is inconvenient for them. Relationships are about trust and compromise and if wearing condoms is where the compromise starts to come apart, I’d start giving your relationship a really hard look.
Stay tuned for the next chapter and thanks for reading!

Resources to Check Out:
The Turnaway Study: https://www.ansirh.org/research/ongoing/turnaway-study
National Health Statistics Report on Contraceptive Use: https://www.cdc.gov/nchs/data/nhsr/nhsr195.pdf
USA Facts data sheet on abortions in the U.S.: https://usafacts.org/articles/how-far-into-pregnancy-do-most-abortions-happen/
NCHS Report on current contraceptive use: https://www.cdc.gov/nchs/data/databriefs/db539.pdf
PubMed NIH article on abortion restrictions threatening miscarriage management: https://pmc.ncbi.nlm.nih.gov/articles/PMC11596537/
CDC report on abortion surveillance report: https://www.cdc.gov/reproductive-health/data-statistics/abortion-surveillance-findings-reports.html
CDC report on emergency contraception: https://www.cdc.gov/nchs/products/databriefs/db112.htm

Leave a comment